
Axial Disc Decompressive Traction Therapy
Research indicates the discs may be responsible for a significant percent of lumbar/leg and neck/arm pain.
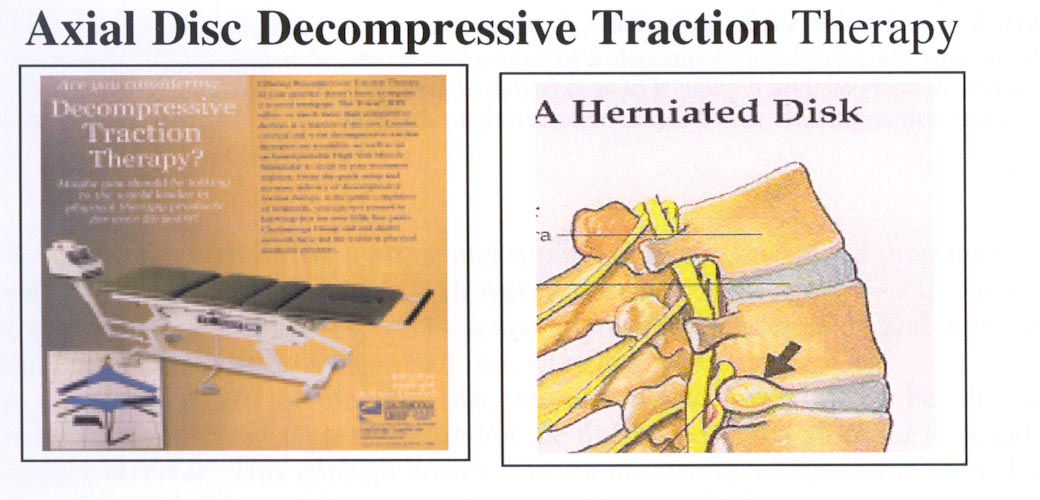
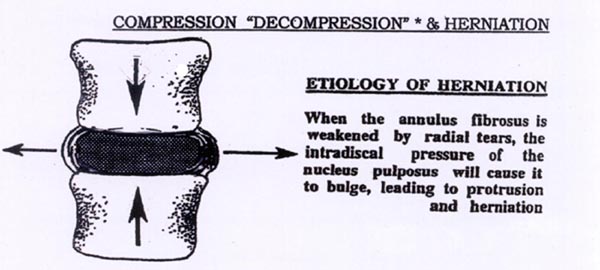
Simply stated, compression (and flexion) increase end-plate, disc (and facet) stress and can lead to inflammatory responses, damage, annular compromise (circumferential and radial tears) and possible extrusion of nuclear material.
Research also indicates not all disc pain can be diagnosed by static imaging (MR) nor do the majority of those with MR findings have pain (as many as 29% of prolapsed discs are not generating pain at the time of the MRI). In theory many mechanical discogenic pathologies can be treated with DTS axial decompression. (For our purposes decompression refers to a reduction of intradiscal pressure and a centripetal effect that improves osmotic exchange, circulation and thus healing).
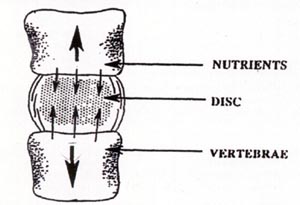
Since the disc is an avascular structure, it doesn't receive fresh blood and oxygen with every beat of the heart. Bogduk reports nutrient supply to the disc is "barely adequate for normal requirements" and the disc's inner portion has the most precarious nutrient supply. Discs require diffusion created by motion and pressure reducing positions to restore nutrients and enhance healing.
Typically back pain with referral pain is an indication for decompression and reduction of those referral symptoms an excellent clinical sign it is working.
However studies suggest some prolapsed and severely degenerated discs may have negative IDP due to a disturbed hydrostatic mechanism. In these cases creating negative IDP by traction to gain a centripetal effect becomes more nebulous (but as long as no increase of symptoms occurs treatment is still warranted for a test period of a few weeks).
Generally in cases with a patent annulus (the disc's outer annulus is still 'intact') centralization of pain can be an excellent clinical indication the treatment is viable.
Centralization is a recognized prognosticator of good clinical outcomes in disc cases. Patients often report centralization during or soon after a DTS treatment thus giving the clinician a viable indicator for a good prognosis and reducing the potential for surgical intervention.
Recumbent positions (both prone and supine) decrease intradiscal pressures in comparison to standing and sitting 3. However, focused, mechanical Y- axis traction improves the discs' healing response via decompression more quickly and with fewer disuse side-effects than prolonged bed rest. 6,7,8,9,10.35,36,40.41,44. There is a suggestion in the literature that extruded nuclear material may be "drawn in" by the reduction of intradiscal pressures and/or the tightening of the posterior longitudinal ligament. 9,10,14,19,44 This concept however is not uniformly accepted due to the limited number of studies able to differentiate the natural history of disc herniation vs. the direct effect of treatment. 1,5,37 Of course whether the disc is the sole source or just a component of the pain is often impossible to prove in many cases.
Many authorities conclude it's not so much something is structurally improved, but an inflammatory response to injury or foreign matter is reduced. We must keep in mind also that many studies suggest less than 5% of patients are good surgical candidates and many back surgeries (and injection procedures) fall to show any long-term value. 5 Thus passive non-surgical procedures that limit side effects and allow progression to active care should be the focus of treatment in that population of patients who fail to improve on their own.
As a passive therapy decompression has definite limitations in curing chronic musculoskeletal conditions. 1,12,14,27,39 Its' value is most specifically in helping discogenic back/neck and referral pain, not acute muscular back pain or those related to posture etc. (other types of therapeutic intervention may be more appropriate). 1,19, Loss of local muscle control & endurance, abnormal posture, cyclical flexion with compression (not to mention genetic influences) are the probable source of most disc damage and degeneration. 48 A passive therapy therefore has little effect truly fixing the underlying problem.
However, a temporary reduction in intradiscal pressure through cyclical stretching can apparently have a profound effect on the healing process via increased contact with the blood/nutrient supply and cellular migration (so called phasic, non-linear effects) as well as neurological changes generated by soft tissue stretch. 8, 9,19,36,44 Decompressive traction of a 'compressive disc lesion' matches treatment to diagnosis and as such is a very reasonable passive therapy.